
Prof. Dr. Murat Demirel, one of the best orthopedic doctors treating hip fractures in elderly patients in Ankara, stands out with his many years of experience in the diagnosis and treatment of this serious orthopedic problem, which is common in the elderly. Hip fractures in elderly patients usually occur as a result of falls, osteoporosis, or trauma, and if not treated properly and on time, they can lead to permanent loss of mobility, decreased independence, and deterioration of overall health. Among the hospitals in Ankara where elderly hip fracture treatment is performed, Prof. Dr. Demirel provides personalized surgical or non-surgical treatment plans for his patients in centers equipped with advanced medical technology and high hygiene standards.
During the treatment process, depending on the type of fracture, the patient’s overall health, and bone quality, prosthetic surgery, fixation with plates and screws, or conservative methods are applied. Following hip fracture treatment in elderly patients, the aim is for recovery to proceed quickly, safely, and with as much independence in mobility as possible, guided by medical recommendations. In addition, transparent and up-to-date information about hip fracture treatment costs in Ankara is provided to help patients and their families make informed decisions. You can also contact us immediately to schedule an appointment and ensure your loved ones recover safely while improving their quality of life.
| Disease Name | Hip Fracture (Elderly) |
| Affected Area | Femoral neck, intertrochanteric region, or subtrochanteric region |
| Symptoms | Sudden hip pain, inability to stand, external rotation of the leg, restricted movement |
| Diagnosis Methods | Physical examination, X-ray, CT, or MRI imaging |
| Causes | Falls (most common), osteoporosis, muscle weakness, balance disorders |
| Risk Factors | Old age, osteoporosis, history of falls, malnutrition, vision problems |
| Treatment Methods | Surgery (internal fixation, prosthesis), physical therapy, pain management |
| Surgical Options | Dynamic hip screw, intramedullary nail, total or partial hip replacement |
| Complications | Deep vein thrombosis, pneumonia, infection, bedsores, mortality |
| Recovery Process | 6–12 weeks post-surgery; intensive rehabilitation may be required |
| Prevention Methods | Fall prevention strategies, osteoporosis treatment, home safety modifications |
| Follow-Up | Regular orthopedic check-ups, physical therapy program, lifestyle modifications |


Prof. Dr. Murat Demirel
Orthopedics and Traumatology Specialist
Orthopedics Specialist Prof. Dr. Murat Demirel was born in Ankara in 1974. He completed his primary education at Ankara Kavaklıdere Primary School and his secondary and high school education at Ankara Atatürk Anatolian High School. Dr. Demirel graduated from Ankara University Faculty of Medicine in 1998 and completed his residency in Orthopedics and Traumatology at Ankara Numune Training and Research Hospital, 1st Orthopedics and Traumatology Clinic, in 2004.
PhD
Ankara University Institute of Health Sciences
Specialization
Ankara Numune Training and Research Hospital, 1st Orthopedics Clinic
Medical School
Ankara University Faculty of Medicine
Yazı İçeriği
Why Are Hip Fractures So Common in Elderly Patients and Which Risk Factors Ring the Alarm Bells?
To understand why hip fractures are so common in the elderly, it is enough to know a simple formula: Fall + Weak Bone = Fracture. When a young person falls, they usually just bruise and get back up. But for an elderly individual, the same fall can result in a life-changing fracture. Why? Because over time our bones undergo changes.
The leading cause of this change is osteoporosis, commonly known as bone loss. We can compare the structure of healthy bone to a tightly woven honeycomb. In osteoporosis, however, the honeycomb spaces widen, the walls thin, and the bone becomes fragile like chalk. In this condition, even a minor household accident like tripping on a rug can be devastating.
Understanding the factors that increase this risk is the first step in prevention. Some factors are beyond our control.
Uncontrollable Risk Factors include:
Advanced Age: As the years pass, our bone density decreases, as do abilities such as balance and muscle strength. This is an inevitable natural process.
Female Gender: Women, especially after menopause, lose bone density much faster due to the decline of the protective effect of estrogen. Therefore, hip fractures are much more common in women than in men.
Genetic Predisposition: If there is a history of hip fracture in your family, especially in your mother or father, your risk may also be higher.
Previous Fracture History: If you have previously experienced a fracture with a simple trauma, such as a wrist or spine fracture, this indicates weak bones and is a red flag for a future hip fracture.
Fortunately, many risk factors are under our control and can be managed.
Modifiable Risk Factors include:
Lifestyle and dietary habits are the most important determinants of bone health. Inadequate calcium and vitamin D intake deprives bones of their building blocks. If calcium is the brick of the bone, vitamin D is the mason placing those bricks; one is useless without the other. Smoking damages bone-building cells and impairs calcium absorption. Excessive alcohol consumption also negatively affects bone health. A sedentary lifestyle not only weakens muscles but also signals to bones that they have no reason to stay strong. Bones only strengthen when they are loaded.
Some chronic diseases also predispose to hip fractures. For example, diabetes impairs bone quality and causes neuropathy, leading to balance problems. Hyperthyroidism, kidney, and liver diseases also directly affect bone metabolism. Neurological diseases such as Parkinson’s, stroke, or dementia dramatically increase the risk of falls.
The medications we use are not always innocent either. Sleeping pills, sedatives, some antidepressants, and antipsychotics can cause dizziness and imbalance, leading to falls. Long-term corticosteroid use is one of the most well-known medication-related causes of osteoporosis.
Situations and habits that significantly increase the risk include:
- Low body mass index (underweight)
- Inadequate protein intake
- Vision and hearing problems
- Orthostatic hypotension (sudden drop in blood pressure upon standing)
- Vitamin B12 deficiency
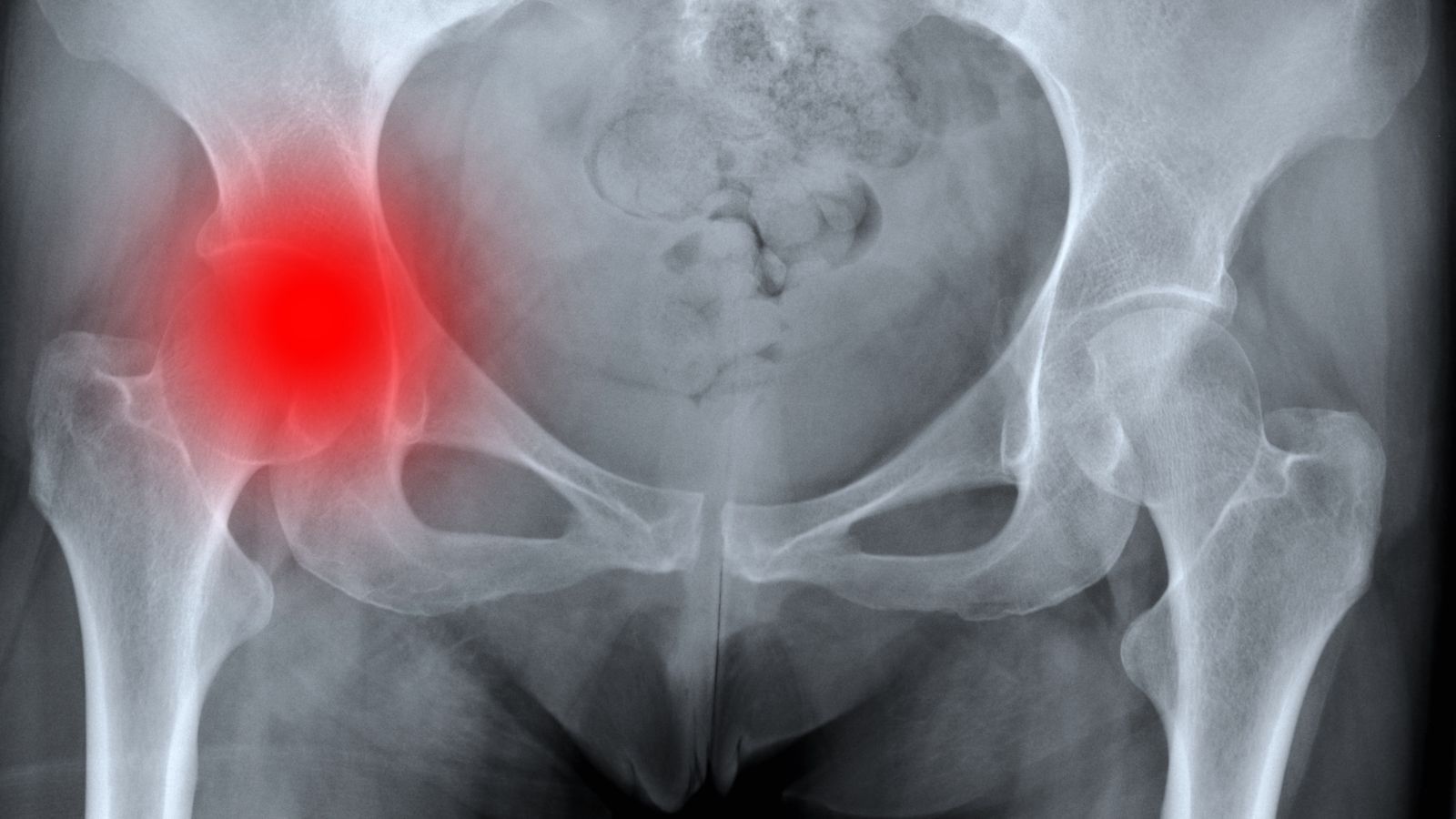
What Symptoms Appear in Elderly Patients with Hip Fractures and How Is the Diagnosis Made?
The warning signs of a hip fracture are usually very typical and occur suddenly after a fall. Recognizing these symptoms is vital for family members so that the patient receives proper medical care immediately. Often, the patient is found lying on the floor in pain after a minor fall.
The most common symptoms requiring an immediate call to emergency services are:
- Inability to get up after a fall
- Severe pain in the hip or groin area
- Inability to bear weight on the affected leg
- Outward rotation of the broken leg
- The broken leg appearing shorter than the other
- Rapid swelling and bruising around the hip
Sometimes, in what is colloquially called a “hip crack,” symptoms may not be as severe. The patient may still walk a few steps with less pain. However, medically, a “crack” is an incomplete or undisplaced fracture and should be treated with the same seriousness. If the patient continues to put weight on it, this “crack” may turn into a full fracture, making treatment much more complicated.
The diagnosis process usually begins in the emergency room when the patient is brought in by ambulance. After the initial examination, an X-ray is taken to confirm suspicions. Most hip fractures are easily diagnosed with a standard X-ray. However, sometimes, especially with undisplaced or incomplete fractures, the X-ray may appear normal. This is called an “occult fracture.” If the patient continues to experience severe pain and inability to bear weight despite a “normal” X-ray, further imaging such as MRI or CT, which provide more detailed images of the bones, is necessary to avoid missing the fracture.
What Surgical Treatments Are Applied for Hip Fractures in Elderly Patients and When Should Surgery Be Performed?
When an elderly patient is diagnosed with a hip fracture, treatment is almost always surgical. The question “Can it heal without surgery?” is often asked, but the risks of non-surgical treatment far outweigh its benefits. Without surgery, the patient remains bedridden for months. This immobility invites a series of potentially fatal complications such as pneumonia, deep vein thrombosis, bedsores, and muscle wasting. Therefore, the modern approach is to operate as soon as possible and mobilize the patient quickly.
The timing of surgery is critically important. The gold standard is to perform the surgery within 24 to 48 hours after hospital admission, provided the patient’s overall condition allows. This early intervention reduces the risk of complications and speeds up recovery.
The surgical method applied depends on the location of the fracture and the patient’s general condition. There are two main surgical approaches.
Fracture Fixation (Osteosynthesis): If the fracture is outside the joint capsule and in a region with good blood circulation, this method may be chosen. Just like gluing the pieces of a broken vase, the bone fragments are repositioned and fixed with special medical devices. Some methods used for this fixation are:
- Dynamic hip screw and plate
- Proximal femoral nail (inserted into the bone)
- Cannulated screws
Joint Replacement (Prosthesis/Arthroplasty): If the fracture is in the femoral head and displaced, the blood supply to this part is disrupted. A bone fragment without blood supply cannot heal. In this case, instead of trying to fix the broken piece, the best approach is to remove it and replace it with an artificial joint, a prosthesis. This can be compared to replacing a damaged car tire that cannot be repaired with a new one. Types of prosthesis surgeries include:
Partial Prosthesis: Only the broken femoral head is replaced. This method is generally preferred for older, less active patients.
Total Hip Replacement: Both the femoral head and the socket in the pelvis are replaced with artificial parts. For younger, more active elderly patients, this provides a more durable and functional solution.
The surgeon decides on the most appropriate treatment by evaluating the patient’s age, bone quality, pre-fracture activity level, and the type of fracture.
Contact us for detailed information and an appointment!
How Does the Recovery Process Progress After Hip Fracture Surgery in Elderly Patients and Which Complications Should Families Watch Out For?
A successful surgery is only the first step of the recovery journey. The real marathon begins after the operation, and in this process, the family’s observation and support are invaluable. It is not only the patient’s bone that needs healing but also the whole body and mind.
The first days after surgery are spent in the hospital. Our goal is to get the patient up with the help of a physiotherapist within the first 24 hours, the day after surgery. This “early mobilization” is our most effective medicine against many complications. The hospital stay usually lasts around a week. However, there are some potential dangers, or complications, that families need to be very careful about during this time.
The most important complications and warning signs that families should know and monitor are as follows:
Delirium (Acute Confusion): This is the most common complication in elderly patients after hip fractures and the one that frightens families the most. The patient may suddenly forget where they are, experience hallucinations, or become agitated or, on the contrary, excessively sleepy. This is not “going crazy”; it is the brain’s temporary response to anesthesia, surgical stress, pain, and unfamiliar surroundings.
Warning signs include:
- Nonsensical speech
- Mixing up dates or people
- Seeing or hearing things that are not there
- Extreme restlessness or unusual calmness
- Inability to distinguish between day and night
Deep Vein Thrombosis (DVT) and Pulmonary Embolism: Due to immobility, blood clots may form in the leg veins (DVT). The dangerous part is when these clots break off and travel to the lungs (Pulmonary Embolism), creating a life-threatening situation.
Warning signs include:
- Sudden swelling, redness, and warmth in the leg (sign of DVT)
- Sudden shortness of breath (the most important sign of PE)
- Chest pain
- Bloody cough
Infections: During this weakened period, infections can easily develop. They are most commonly seen at the surgical site, in the lungs (pneumonia), and in the urinary tract.
Warning signs include:
- Redness, discharge, and warmth at the surgical site (wound infection)
- Fever, cough, green-yellow sputum (pneumonia)
- Frequent urination, burning, foul odor (urinary tract infection)
Pressure Sores (Bedsores): These occur due to continuous lying down, especially in areas over bony prominences such as the sacrum or heels, where skin blood supply is compromised. The best prevention is frequent position changes and early mobilization.
Why Are Physical Therapy and Rehabilitation Essential After Hip Fractures in Elderly Patients, and What Should Be Expected in the Process?
“Doctor, the surgery is done, now what? When will they walk again?” This is the most common question we hear from relatives. The answer is clear: now begins the most important and longest stage of recovery—rehabilitation. Surgery repairs the broken bone, but what will get the patient walking again and restore their strength and independence is physiotherapy.
Rehabilitation begins the day after surgery with simple exercises at the bedside and continues for months, sometimes even over a year. This is a marathon and requires patience. The process usually continues after hospital discharge, either in a rehabilitation clinic or with home care services.
The cornerstones of a comprehensive rehabilitation program are:
Muscle Strengthening Exercises: Aim to rebuild weakened hip and leg muscles due to surgery and immobility.
Balance and Coordination Training: Critical to overcome fear of falling and to regain confident steps.
Walking Training: A gradual process starting with a walker, then a cane, and eventually independent walking.
Daily Living Activity Training: Occupational therapists teach patients how to safely perform daily tasks such as dressing, bathing, and cooking simple meals again.
It is important to have realistic expectations during this process. Not every patient can return to their pre-fracture functional level. The goal is to maximize the patient’s potential and ensure as independent and quality a life as possible. Every step taken and every small success achieved is a great victory and should be celebrated.
How Can Future Hip Fractures in Elderly Patients Be Prevented and the Risk of Falls Reduced?
Treating a hip fracture is difficult, but preventing it is both easier and much wiser. Especially for individuals who have already had a fracture or are in the risk group, preventive measures are not optional but mandatory. Prevention strategies can be divided into two main pillars: strengthening bones and preventing falls.
Pillar: Protecting and Strengthening Bones
This is where we fight osteoporosis. There are steps we can take to make our bones stronger.
Nutrition is the most basic step. Bone-friendly foods must be included in your diet.
Rich sources of calcium include:
- Milk, yogurt, kefir
- Cheese (especially low-salt varieties)
- Dark green leafy vegetables (spinach, broccoli, arugula)
- Almonds
- Molasses
- Legumes
Vitamin D is the “sun vitamin.” Our body produces it when our skin is exposed to sunlight. Exposing arms and legs to the sun for 15–20 minutes during non-peak hours (morning or late afternoon) is important. However, since the body’s ability to produce vitamin D decreases with age, supplementation is often necessary under medical supervision.
If bone density testing reveals osteoporosis, diet and supplements alone may not be sufficient. In this case, prescription medications that slow bone resorption or increase bone formation and can reduce fracture risk by up to 50% may be needed.
Pillar: Preventing Falls
No matter how strong your bones are, frequent falls always carry a risk of fractures. About 90% of falls occur at home or nearby. Therefore, we must turn our homes into safer places for the elderly.
Simple but effective home safety modifications include:
- Remove small rugs, mats, and cables that can cause tripping.
- Improve lighting in rooms and corridors, use night lights.
- Install sturdy grab bars in bathrooms and toilets.
- Place non-slip mats on bathroom floors and inside showers.
- Ensure staircases are well-lit and non-slippery.
- Store frequently used items on easily accessible shelves and avoid stools for reaching high places.
Proper footwear is also very important. Shoes that fit well, have non-slip soles, and fasten securely should always be worn indoors and outdoors. Slippers, especially backless ones, are among the most dangerous causes of household accidents.
Regular exercise is our strongest weapon in preventing falls. Exercises that increase muscle strength and balance significantly reduce fall risk. It is best to develop a personalized exercise program with the help of a physiotherapist.
Finally, regular eye and hearing check-ups should be done, and all medications the patient uses should be reviewed periodically by a physician for potential side effects causing dizziness.
Why Is a Multidisciplinary Team Important in the Management of Hip Fractures in Elderly Patients?
In the past, hip fractures were considered a problem only for orthopedic specialists. But now we know that a hip fracture in an elderly patient is just the tip of the iceberg. Underlying problems such as diabetes, heart failure, malnutrition, and dementia often coexist, and all of these are interconnected. That is why the best outcomes are achieved with a team of specialists from different fields working together.
This modern care model, called the “orthogeriatric” approach, has the patient and family as the conductors of the orchestra. The other team members are:
Orthopedics and Traumatology Specialist: The surgeon responsible for the proper repair of the fracture.
Geriatric Specialist: Manages all other medical issues, organizes medications, plans nutrition, and plays a key role in preventing complications such as delirium.
Physiotherapist: Helps the patient regain muscle strength, balance, and walking ability.
Anesthesiologist: Plans the safest anesthesia while considering the delicate balance of the elderly patient.
Nurses: Provide 24/7 care for the patient, often the first to detect and respond to complication signs.
Dietitian: Develops a nutrition program rich in protein, calcium, and vitamins essential for fracture and wound healing.
Contact us for detailed information and an appointment!
Frequently Asked Questions
How do hip fractures occur in elderly patients and who is more at risk?
Hip fractures in the elderly usually occur after a simple fall and are more common in women with osteoporosis (bone loss). Aging increases bone weakness and balance problems, while muscle loss and vision issues are also major risk factors.
What are the symptoms of a hip fracture?
Sudden pain in the hip, groin, or thigh, deformity, shortening of the leg, external rotation, inability to stand, or inability to bear weight are the main symptoms. Sometimes the symptoms may present as mild pain.
How is a hip fracture diagnosed?
Diagnosis is made with a physical examination and reviewing the patient’s fall history. X-rays identify the type and location of the fracture. In uncertain cases, especially if fractures are not visible on X-ray, advanced imaging methods such as CT or MRI are used.
Is surgery mandatory for hip fractures in the elderly?
Surgery is required in most hip fracture cases. Surgery restores the position and fixation of broken bones. In special cases, when surgery is not possible or if the patient’s condition is very poor, casts, splints, or bed rest may be considered.
What is the recovery process after surgery?
Early mobilization after surgery is very important in elderly patients. Most patients are mobilized within a few days with physical therapy support. Recovery time varies depending on age, general health, and fracture type, but returning to independent living may take 2–3 months.
How does a hip fracture affect life in the elderly?
Hip fractures cause loss of mobility and independence in the elderly. Long-term bed rest can lead to severe complications such as pneumonia, bedsores, and vascular clots. Depression and social isolation are also common.
Is walking possible again after a hip fracture?
With successful surgery and regular physiotherapy, most elderly patients are able to walk again. However, regaining walking ability depends on the patient’s overall condition, muscle strength, and bone health.
What should be considered in post-fracture care?
Wound care, prevention of bedsores, adequate nutrition, frequent position changes, and hygienic management of toileting are very important. Muscles should be strengthened with physical therapy exercises.
Is hip fracture surgery risky in elderly patients?
Due to advanced age and comorbidities (heart disease, diabetes, hypertension, etc.), the risks of surgery are higher. However, long-term bed rest without surgery carries far greater risks. Therefore, surgery is generally recommended.
How can hip fractures in the elderly be prevented?
Osteoporosis treatment, balanced nutrition, regular exercise, fall-prevention measures at home (non-slip rugs, good lighting, grab bars), regular eye check-ups, and proper footwear choices reduce the risk of hip fractures.
Blog Posts

What Is a Tendon Rupture? Symptoms, Causes, and Treatment Methods
Ankara Ortopedi | Prof. Dr. Murat Demirel » General » What Is a Tendon Rupture? [...]
13
Apr
Apr

What Is an Orthosis? Why Is an Orthosis Used?
Ankara Ortopedi | Prof. Dr. Murat Demirel » General » What Is an Orthosis? Why [...]
13
Apr
Apr

Knee Replacement Surgery Prices
Ankara Ortopedi | Prof. Dr. Murat Demirel » Knee Treatments » Knee Replacement Surgery PricesThe [...]
18
Aug
Aug

Hip Replacement Surgery Prices
Ankara Ortopedi | Prof. Dr. Murat Demirel » Hip Treatments » Hip Replacement Surgery PricesThe [...]
18
Aug
Aug